Lichen planus (LP) is an immune-mediated disease with an unknown etiology. Its clinical presentation waxes and wanes, and its severity goes from symptomatic oral erosions with erythema to asymptomatic white striations. In the oral cavity, the locations of these clinical signs are more commonly found symmetrically and bilaterally, usually in the buccal mucosa, tongue (dorsal, ventral, lateral), gingiva (buccal and lingual), posterior vestibule, labial mucosa, lips, and less commonly present in the floor of the mouth and palate [1]. Also, it can be present in esophageal, laryngeal, nasal, conjunctival, anal, and genital mucous membranes, skin, nails, and scalp. [2] Careful examination of the surface of the skin papules (Figure 1) reveals a fine, lacelike network of white lines (Wickham’s striae). [3]

Figure 1. Patient with biopsy-proven oral lichen planus with skin lesions.
The prevalence of OLP worldwide ranges from 0.22 to 5% 1, and locally, specifically in Los Angeles, California, at The Orofacial Pain and Oral Medicine Center of the University of Southern California, represents the 10th most common diagnosis (out of over 200 diagnoses). Frequently, the patient presents an associated burning sensation with foods, including but not limited to spicy or acidic food. [1]
Like what you’re learning? Download a brochure for our online, postgraduate Oral Pathology and Radiology certificate program.
There are three most common clinical presentations of oral lichen planus: erosive, reticular, and plaque-like. [4]

- Erosive lichen planus (Figure 2), although not as common as the reticular form, is more significant for the patient because the lesions are usually symptomatic. Clinically, there are atrophic, erythematous areas with central ulceration of varying degrees. The periphery of the atrophic regions is usually bordered by fine, white, radiating striae.
Figure 2. Clinical presentation of Erosive Lichen Planus on the left lingual gingiva of the mandibular teeth
- Reticular lichen planus (Figure 3) is much more common than the erosive form, usually asymptomatic.
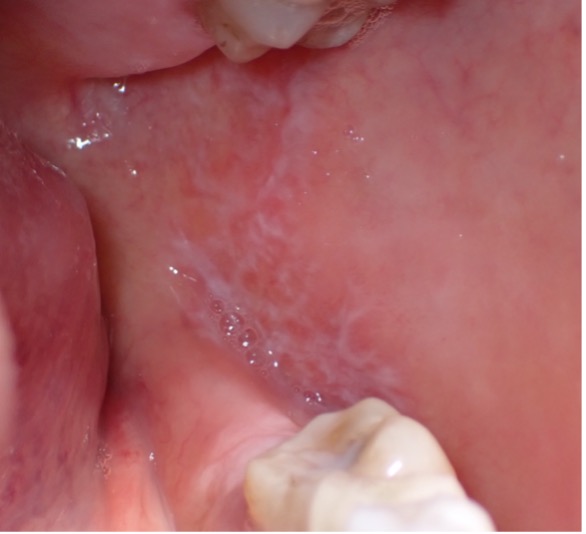
Figure 3. Patient presenting bilateral reticular lesions typical of oral lichen planus; in addition, some erosive lesions appear in the left buccal mucosa. [5]
- Plaque-like (Figure 4) usually asymptomatic, and the common location is the dorsal tongue.

Figure 4. A patient presented with plaque-like lesions on the dorsal tongue and biopsy-proven lichen planus.
How to Manage OLP?
Dentists, oral pathologists, and oral medicine practitioners are usually the most common providers who will manage these patients; a biopsy will be performed for definitive diagnosis and to rule out other conditions with similar clinical presentation, and the focus of the OLP therapy will be controlling the symptoms. Patients with reticular lesions and other asymptomatic lesions do not require active treatment. Still, the elimination of potential precipitating or provoking factors (sharp or fractured teeth, incongruous dental prostheses, alcohol, and tobacco consumption) is fundamental. Although there is no permanent cure therapy, various treatment regimens have been introduced to reduce and control the painful symptoms of OLP. [2]
With topical corticosteroids such as super-potent halogenates and calcineurin inhibitors, it is possible to obtain a safe and satisfactory control of the symptoms caused by OLP lesions in most cases. [2] Some studies report that the use of corticosteroids (during the acute phase) may have a protective effect on the onset of the cancer itself. But these same drugs, due to their immunosuppressive effects, could themselves be promoters of the onset of oral cancer.
Some new treatment modalities are potentially interesting for cases refractory to conventional therapies, such as the oxygen-ozone mixture injections. [2]
Other specialists involved in the care of lichen planus patients are dermatologists who specialize in diagnosing and treating skin conditions, including lichen planus.
So, when should you consider referring for dermatologist evaluation a lichen planus patient? (Below are some cases to consider.)
- Patients with possible lichen planus skin lesions presenting with unusual changes in the skin, such as the development of purple, flat-topped bumps or lesions with fine white lines over them, it’s a good idea to consult a dermatologist [5].
- Patient with oral and genital involvement: Lichen planus can also affect the mucous membranes, including the mouth and genital areas. Patients may experience pain or unusual lesions in these areas [6].
- Itching and discomfort in the skin: Lichen planus can be associated with itching, and if the symptoms are bothersome or affect your quality of life, a dermatologist can help determine the appropriate treatment [5, 6].
- If topical medications are not effective for managing oral symptoms and if there is a history of systemic previous treatment failures, a dermatologist may provide additional care and treatment options [7].
Interdisciplinary management is approached on multiple levels. First and foremost, the patients appreciate the combined expertise and intensified care. Moreover, the collaboration is cost and time-efficient and again improves patient satisfaction. Furthermore, there is a mutual learning benefit when it comes to different approaches to disease management. Dermatologists become more familiar with dental health, and dentists receive insight into systemic immunomodulatory treatment approaches and extraoral manifestations of the disease. [5, 6, 8]
Conclusion
If you suspect the presence of skin lesions in oral lichen planus are experiencing persistent skin changes, discomfort, or other associated symptoms, or the patient is not responding to the conventional treatment it is crucial to consult with a dermatologist. Dermatologists are specialized healthcare professionals equipped to accurately diagnose and effectively treat various skin conditions, including lichen planus. Timely intervention and expert guidance can help manage symptoms, alleviate discomfort, and improve overall quality of life. It is worth mentioning that the advantages of a joint clinic include a holistic approach focusing on dental and skin health at the same time, enhancing patients’ confidence in receiving the optimal
treatment strategy and increasing compliance.
Postgraduate Oral Pathology and Radiology Certificate
Learn more about the clinical and didactic skills necessary to evaluate and manage patients with oral diseases by enrolling in Herman Ostrow School of USC’s online, competency-based certificate program in Oral Pathology and Radiology.
References
- Vistoso, Anette 2023, Can Oral Lichen Planus (OLP) look like Oral Epithelial Dysplasia? Herman Ostrow School of Dentistry of USC, accessed 16 February 2024, https://ostrowonline.usc.edu/can-oral-lichen-planus-olp-look-like-oral-epithelial-dysplasia/.
- Isola, Gaetano; Santonocito, Simona; Leonardi, Rosalia ; Polizzi, Alessandro. Oral Lichen Planus and Lichenoid Lesions: Etiopathogenesis, Diagnosis and Treatment. DOI: 10.1007/978-3-031-29765-6. Springer Nature-Springer English International eBooks 2023.
- Neville B.W, Damm D.D, Allen C.M, Bouquot, J.E Oral and Maxillofacial Pathology, 3rd ed. St Louis: Elsevier-Saunders. 2009; St Louis: Elsevier. ISBN: 978-1-4160-3435-3
- Wagner, Gunnar; Rose, Christian; Sachse, Michael Max Clinical variants of lichen planus DOI: 10.1111/ddg.12031 Germany: Blackwell Publishing Ltd Journal der Deutschen Dermatologischen Gesellschaft, 2013, Vol.11 (4), p.309-319.5.
- Ioannides D, Vakirlis E, Kemeny L, Marinovic B, Massone C, Murphy R, Nast A, Ronnevig J, Ruzicka T, Cooper SM, Trüeb RM, Pujol Vallverdú RM, Wolf R, Neumann M. European S1 guidelines on the management of lichen planus: a cooperation of the European Dermatology Forum with the European Academy of Dermatology and Venereology. J Eur Acad Dermatol Venereol. 2020 Jul;34(7):1403-1414. doi: 10.1111/jdv.16464. PMID: 32678513.
- Khurana A, Tandon S, Marfatia YS, Madnani N. Genital lichen planus: An underrecognized entity. Indian J Sex Transm Dis AIDS. 2019 Jul-Dec;40(2):105-112. doi: 10.4103/ijstd.IJSTD_45_19. PMID: 31922099; PMCID: PMC6896385.
- https://www.aad.org/public/diseases/a-z/lichen-planus-treatment
- Pawlowski J, Beczinski J, Stege H, et al. Bridging the gaps: management of lichen planus subtypes in a joint dermatology-oral surgery clinic. Clinical and experimental dermatology. 2023;49(1):18-25. doi:10.1093/ced/llad335
