Chronic Trigeminal Neuropathy
Chronic trigeminal neuropathy (CTN) involves damage or dysfunction of the trigeminal nerve, which is responsible for transmitting sensory information from the skin and mucosal surfaces of the face to the brain. Depending on the severity and location of the nerve damage, this condition can lead to symptoms such as numbness, tingling, burning sensations, or facial pain [1]. All these symptoms can interfere with and affect the patient’s quality of life in several ways.
What are the possible causes?
CTN can occur due to several causes, including trauma, infections (such as herpes zoster), multiple sclerosis, vascular compression, or iatrogenic injury from surgical procedures or dental work. Unlike trigeminal neuralgia, which involves short (seconds to minutes) episodic, sharp, electric-like pain affecting one or more branches of the trigeminal nerve, CTN often manifests as continuous pain or sensory disturbances [1].
Like what you’re learning? Download a brochure for our Orofacial Pain and Oral Medicine certificate or master’s degree program.
Some treatment options are available below and in Table 1.
- Non-pharmacological methods
CTN treatment includes non-pharmacological methods, such as TENS units for pain relief, botulinum toxin injections targeting nerve areas, and neurosensory gingival stents for pain in the oral mucosa (Figure 1).
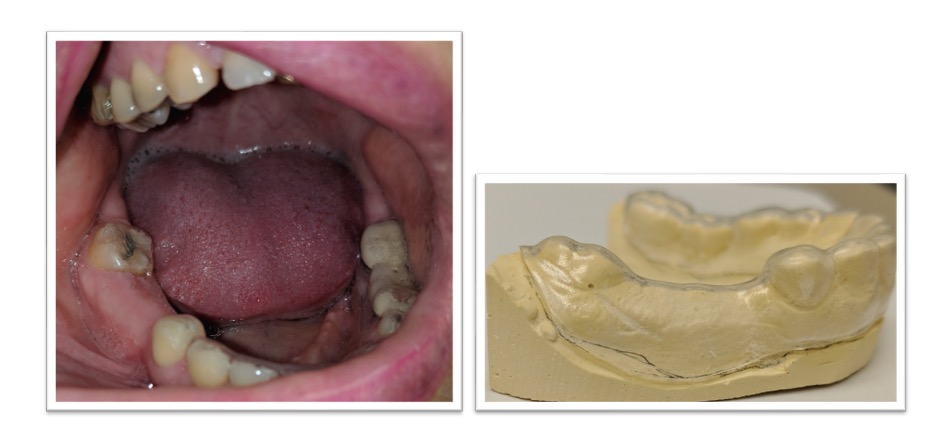
Figure 1: Showed the right mandibular edentulous ridge of a patient diagnosed with CTN and the fabricated stent to cover the painful site
- Pharmacological methods
Pharmacological treatments include antidepressants (e.g., SSRIs, SNRIs, TCAs) and anticonvulsants (e.g., gabapentin, carbamazepine), which suppress neuronal hyperexcitability. [2]
Table1. Treatment plan according to symptoms patients report after the assessment and diagnostic tests.
| Symptoms | Treatment Plan |
| 1. Pain due to local cause (compression, dental source, etc.) | Occlusal appliance to stop occlusal compression, refer for dental treatment |
| 2. Focal Allodynia (pain in a specific site from stimuli that are typically non-painful) | Apply daily topical anesthetic and consider stent |
| 3. Pain with anxiety and somatically focused (attention concentrated on physical sensations or bodily symptoms) | Prescription: SNRI (e.g. duloxetine), TCA (e.g. amitryptiline) |
| 4. Pain is not completely relief with topical medication | Daily topical anesthesia with or without stent + Anticonvulsant |
| 5. Not effective previous treatments | Consider intraosseous injections of depomedrol, combinations of medications, refer to pain psychologist. |
Definitions: SNRI= Serotonin-norepinephrine reuptake inhibitors; TCA= tricyclic antidepressant.
Vitamin B12 and Alpha Lipoic Acid
In recent years, researchers have explored the use of Vitamin B12 and Alpha Lipoic Acid (ALA), both of which are known to reduce inflammation and oxidative stress in the body. These over-the-counter resources offer promising potential in supporting nerve regeneration and overall health.
- Vitamin B12 is essential for nerve function due to its role in metabolizing fatty acids that maintain the myelin sheath, which insulates and protects nerves. A prolonged deficiency in Vitamin B12 can lead to nerve degeneration, resulting in irreversible damage. Research has shown that Vitamin B12 can stimulate nerve regeneration by promoting axon growth, a critical component of recovery following peripheral nerve injury.
- Alpha Lipoic Acid (ALA) plays a significant role in mitochondrial energy production. As a powerful antioxidant, ALA neutralizes reactive oxygen species (ROS) and improves blood flow to nerves, leading to enhanced nerve function and regeneration. Additionally, ALA has been found to improve glucose metabolism and insulin sensitivity in type 2 diabetes patients, offering greater health benefits. [3]
Vitamin B12 and Neuropathy
Vitamin B12 deficiency can cause peripheral neuropathy. Untreated B12 deficiency results in progressive nerve damage, which can eventually become irreversible. Although Vitamin B12 supplementation may not reverse existing nerve degeneration, it can stop further damage and improve symptoms. [3]
Alpha Lipoic Acid and Neuropathy
ALA is widely studied for its role in managing diabetic neuropathy (DN), particularly due to its antioxidant properties. It has shown cytoprotective effects in the nervous system and has been demonstrated to reduce neuropathic pain in clinical trials. A meta-analysis of randomized controlled trials involving 523 patients found that ALA significantly reduced pain and improved nerve function in both type 1 and type 2 diabetes patients. Moreover, ALA has demonstrated the ability to promote nerve regeneration and support overall nerve health. Its anti-inflammatory and antioxidant properties make it an ideal candidate for treating neuropathies like TN. [3]
Vitamin B12 and ALA in Combination Therapy
Combining Vitamin B12 and ALA offers a synergistic effect, tackling nerve damage from multiple angles. While Vitamin B12 repairs and maintains the myelin sheath, ALA reduces oxidative stress and improves blood flow to the affected nerves. This combination may be especially beneficial in patients with trigeminal neuralgia and painful peripheral neuropathy, as it addresses both the inflammatory and regenerative aspects of nerve damage. [4]
The results of various studies have shown the potential of Vitamin B12 in treating post-herpetic neuralgia and painful peripheral neuropathy due to its role in nerve repair. A study found that injectable Vitamin B12 was more effective than oral nortriptyline, a common neuropathic pain treatment, in reducing symptoms such as paresthesia and tingling. This suggests that parenteral B12 may offer superior relief for neuropathic pain compared to standard oral medications. Therefore, maintaining adequate Vitamin B12 levels, alongside ALA supplementation, could prove beneficial in managing CTN. [5]
Conclusion
For patients with CTN, incorporatinB12 and ALA could significantly improve symptoms and prevent further nerve damage. Research indicates that parenteral B12 may offer more effective relief compared to oral options, making it a viable addition to CTN management alongside ALA. Further studies are warranted to solidify their role in protocols for CTN.
Earn an Online Postgraduate Degree in Orofacial Pain and Oral Medicine
Are you interested in a variety of issues focused on orofacial pain, medicine and sleep disorders? Consider enrolling in the Herman Ostrow School of Dentistry of USC’s online, competency-based certificate or master’s program in Orofacial Pain and Oral Medicine.
References
- Eliav T, Benoliel R, Korczeniewska OA. Post-Traumatic Trigeminal Neuropathy: Neurobiology and Pathophysiology. Biology (Basel). 2024 Mar 4;13(3):167. doi: 10.3390/biology13030167. PMID: 38534437; PMCID: PMC10967710.
- Shkodina AD, Bardhan M, Chopra H, Anyagwa OE, Pinchuk VA, Hryn KV, Kryvchun AM, Boiko DI, Suresh V, Verma A, Delva MY. Pharmacological and Non-pharmacological Approaches for the Management of Neuropathic Pain in Multiple Sclerosis. CNS Drugs. 2024 Mar;38(3):205-224. doi: 10.1007/s40263-024-01072-5. Epub 2024 Feb 29. PMID: 38421578.
- Didangelos T, Karlafti E, Kotzakioulafi E, Kontoninas Z, Margaritidis C, Giannoulaki P, Kantartzis K. Efficacy and Safety of the Combination of Superoxide Dismutase, Alpha Lipoic Acid, Vitamin B12, and Carnitine for 12 Months in Patients with Diabetic Neuropathy. Nutrients. 2020 Oct 23;12(11):3254. doi: 10.3390/nu12113254. PMID: 33114210; PMCID: PMC7690794.
- Xu Q, Pan J, Yu J, Liu X, Liu L, Zuo X, Wu P, Deng H, Zhang J, Ji A. Meta-analysis of methylcobalamin alone and in combination with lipoic acid in patients with diabetic peripheral neuropathy. Diabetes Res Clin Pract. 2013 Aug;101(2):99-105. doi: 10.1016/j.diabres.2013.03.033. Epub 2013 May 9. PMID: 23664235.
- McMullin PR, Hynes AT, Arefin MA, Saeed M, Gandhavadi S, Arefin N, Eckmann MS. Infusion Therapy in the Treatment of Neuropathic Pain. Curr Pain Headache Rep. 2022 Sep;26(9):693-699. doi: 10.1007/s11916-022-01071-5. Epub 2022 Jul 6. PMID: 35794449.

